By: Dr. Margarita David Ph.D., RN
Pancreatic cancer affects over 60,000 people in the United States. Continue reading to learn more about pancreatic cancer in honor of Pancreatic Cancer Awareness Month.
Pancreatic cancer is a cancer that develops in the pancreas. The pancreas helps regulate the metabolism of sugar and aids in the digestion of foods.
Although the exact cause of pancreatic cancer is still unknown, some risk factors that may contribute to the development of pancreatic cancer include:
Many of the symptoms of pancreatic cancer are also common with other types of cancers. These may include:
There are several ways that pancreatic cancer is diagnosed:
Three blood tests can help diagnose and treat pancreatic cancer:
If blood work and imaging indicate the possibility of having pancreatic cancer, a biopsy (a tissue sample from the pancreas) is taken to confirm the diagnosis. A biopsy is the gold standard for a definitive pancreatic cancer diagnosis.
Pancreatic cancer can be extremely painful, making your quality of life more difficult toward the end of life. Hospice care allows people to live their final stages in peace by providing:
The end of life can be a very stressful, uncomfortable, and anxiety-provoking time. A hospice team can help provide the comfort the patient needs physically, emotionally, and spiritually.
Hospice care takes care of you physically and emotionally during the end of life. The team consists of a social worker and chaplain who will work with you and your family to ensure your spiritual needs are met. Hospice provides compassionate care that is supportive of both the patient and their families through the end of life and throughout the grieving process.
Caring for sick loved ones can be an exhausting endeavor, which is why hospice care takes over your care so that your family gets a much-needed break. Your hospice team can also coordinate respite periods for your caregiver.

By: Laura Mantine, MD
Chronic lung disease is the 4th most common cause of death among older adults in the United States. More than 3 million people worldwide died of COPD in 2015, representing 6% of all deaths that year. People dying from COPD frequently experience difficult and uncomfortable symptoms that lead to distress and panic. They commonly have disabling respiratory symptoms including severe breathlessness, limited tolerance for activity, and intractable coughing. They are also usually oxygen dependent, often experience anorexia with weight loss, cachexia, and ultimately become dependent on others for their activities of daily living.
Despite the symptomatic needs of individuals dying from end-stage COPD, only 30% of individuals receive hospice care before death. It is not clear why the rate of hospice use for patients with COPD is so low, but several explanations have been offered. The most important may be that few patients with severe COPD have discussed end-of-life planning with their clinician. Furthermore, many patients and clinicians do not view COPD as a terminal illness and feel it is more chronic in nature. Also, there may be a lack of awareness that patients enrolled in hospice can continue to receive treatments for COPD. Due to the fluctuating course of COPD, it is often difficult to accurately estimate a patient’s life expectancy which may contribute to low hospice utilization rates.
While end-of-life-care is an appropriate topic to discuss with all patients, several factors have been suggested that should prompt a discussion with patients who have severe COPD. One factor is simply that a clinician would not be surprised if a patient with COPD were to die within the next 6-12 months. A clinician should consider hospice referral in a patient with COPD if they are dyspneic at rest or with minimal exertion, have progressed to the point where they spend most of their days at home, have experienced repeated ED visits (one or more each quarter) due to infection or episodes of respiratory failure, have endured repeated hospitalizations (one or more each quarter) and no longer wish to be admitted and the patient no longer wishes to be intubated.
While these laboratory studies may be helpful to the clinician when considering patient appropriateness for hospice services, they are not required for patient admission.
COPD is a significant health issue around the world. It is ultimately a fatal disease and patients are under-referred to hospice care. Hospice, with its strong interdisciplinary approach, has been shown to improve quality of life for patients with end-stage respiratory disorders like COPD.
Hospice Eligibility for Patients with COPD. Serena J. Scott, MD, Barry D. Weiss, MD, Ellyn Lee, MD, College of Medicine, University of Arizona. https://uofazcenteronaging.com. June 2017.
When to refer patients with advanced COPD to palliative care services. Rebecca Strutt. Breathe (Sheff). 2020 Sep; 16(3): 200061.
Referral to palliative care in COPD and other chronic diseases: A population-based study. Kim Beernaert; Joachim Cohen; Luc Deliens; Dirk Devroey; Katrien Vanthomme; Koen Pardon; Lieve Van den Block. Respiratory Medicine. Volume 107. Issue 11, P1731-1739. November 1, 2013.

We’ve all heard how good yoga is for you, but have you ever thought about the benefits of yoga for hospice patients? Yoga is defined as a spiritual discipline that is widely practiced for health and relaxation that includes breath control, simple meditation, and specific bodily postures. All of these things can be used to help hospice patients and their families navigate through an emotionally stressful time.
Yoga is a combination of spiritual, mental, and physical practices that originated in ancient India approximately 5,000 years ago. It was originally practiced primarily to cultivate spiritual harmony and enlightenment.
It started to become more popular in the late 1800s as it spread west. New practitioners viewed it as a path to inner peace and better health. Then, we saw what is called the ‘Modern Yoga Renaissance’ in the 1920s where the physical practice of yoga dramatically changed. Prior to this point, it really only consisted of a few standing poses. Today, yoga has become a key component of holistic health.
Learn more about the history of yoga here.
When we think of yoga, we often think of poses like downward dog or child’s pose or even the more complex poses that turn a person into a pretzel. However, before you can learn to twist and turn and pose like that, you must focus on something you already know how to do. In fact, you do it all day, every day: breathe.
In yoga, breath control is referred to as pranayama [pränəˈyämə], and it is essential. There are several forms of pranayama that can be done from the seated position. One example of this is Adham Pranayama. It can be performed either sitting or lying down, whatever is most comfortable. The focus of Adham Pranayama is ‘belly breathing,’ or breathing deeply into your stomach.
So how do you do it, you ask. First, place one hand on your stomach and the other on your chest. Breathe in and out. Focus on moving only your abdomen, instead of inflating your chest. It’s as simple as that. Practicing Adham Pranayama has several benefits, including reducing insomnia, providing oxygen to the body, and relieving stress.
There are many other forms of pranayama that can be done anywhere and in comfortable, seated positions. You can learn more about them here.
Yoga can easily be adapted to fit the needs and ability of the person doing it. Plus, it can be done anywhere- from a yoga studio to the comfort of your own home, even from your bed! Not to mention the benefits of mindful breathing. This can be an incredibly difficult time for patients and their loved ones. Taking time to truly focus on your breathing can provide a break in the stress and anxiety you may be feeling. Plus, it can be done together, helping to reduce everyone’s stress while also creating peaceful memories you’ll have forever.

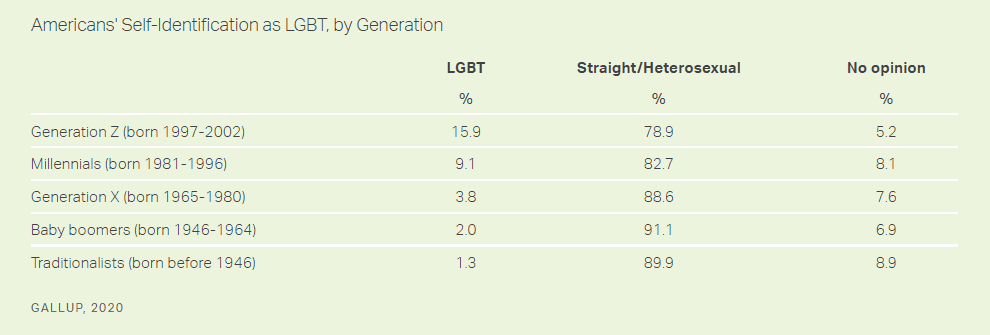 Although those who make up the younger generations were born into a world where huge progress has been made in the gay rights movement, the older generations of the LGBTQ community experienced much less accepting times. It wasn’t until 1961 that Illinois became the first state in the United States to get rid of its sodomy law. It then took another ten years before 20 more states followed their lead. So even though Traditionalists and Baby Boomers were around to witness the progress that has been made, many may still have the mindset that society will not accept them for who they are.
It is this fear of discrimination that may play a part in their hesitation to seek the help and support they need as they near the end of their life. As a result, the LGBTQ community has been historically underserved by hospice. A 2011 study reported that 20% of LGBTQ seniors that were surveyed did not even reveal their sexual orientation to their primary physician for fear of discrimination. Beyond hospice services for the patient, their grieving partner often misses out on bereavement support as they care for their partner in their final months and days.
Although those who make up the younger generations were born into a world where huge progress has been made in the gay rights movement, the older generations of the LGBTQ community experienced much less accepting times. It wasn’t until 1961 that Illinois became the first state in the United States to get rid of its sodomy law. It then took another ten years before 20 more states followed their lead. So even though Traditionalists and Baby Boomers were around to witness the progress that has been made, many may still have the mindset that society will not accept them for who they are.
It is this fear of discrimination that may play a part in their hesitation to seek the help and support they need as they near the end of their life. As a result, the LGBTQ community has been historically underserved by hospice. A 2011 study reported that 20% of LGBTQ seniors that were surveyed did not even reveal their sexual orientation to their primary physician for fear of discrimination. Beyond hospice services for the patient, their grieving partner often misses out on bereavement support as they care for their partner in their final months and days.